
Fixing the hidden time-bomb in hospital bed capacity

Richard Jones, Chief Strategy Officer for C2-AI outlines a solution that could release hospital capacity now and sustainably into the future – while saving 70,000+ lives annually and £900 million.
This article will discuss one of the ‘10 Essential Digital Health ideas for a COVID-19 UK National Response’ (Healthcare UK) and an aspect of care proven in some NHS hospitals, that could free space for more than 11,000 extra Covid-19 patients in NHS England alone over a three month period.
Bed and ventilator capacity are currently being ‘lost’ to patients with avoidable conditions that they acquire in hospital. Patients diagnosed with Acute Kidney Injury (AKI) and Hospital-Acquired Pneumonia (HAP) stay six and eight days longer in hospital respectively.
To make matters worse as we think about capacity for future surges, these conditions are particularly common in ICU. Up to 70 per cent of patients in critical care units have AKI/HAP and these two avoidable conditions account for 1.6m bed days lost in the NHS every year with 360,000 of those in critical care beds.
Before addressing a practical approach that will reduce patients acquiring AKI/HAP, and therefore free up capacity, it’s worth exploring why the impact of these conditions gets worse in surge situations, and so why the solution becomes even more important during these periods.
Although the response and commitment in the NHS is nothing short of magnificent, the quality of care in hospitals has inevitably decreased. Intensive care staffing ratios have reduced, and patients are being treated in parts of hospitals and other facilities that were simply not designed for the task. The cancellation of elective surgery is logical but means the case-mix in hospitals has become more challenging with patients that are generally admitted in reasonable health (where possible) being replaced by seriously ill Covid-19 patients. Patients admitted into hospital will also be presenting in worse condition than normal due to the pressures in primary care. This will also lead to higher readmission rates with patients discharged earlier than normal but returning in extremis.
In simple terms, the already serious impact of these avoidable conditions worsens during any surge. More patients will acquire these avoidable conditions, developing more serious cases on average and so increasing the length of stay. The specialist equipment that is normally sufficient will therefore come under pressure, e.g. AKI patients may well overcome the capacity of existing dialysis machines.
The bottom line is that deaths from these avoidable conditions will worsen during a surge and a greater percentage of capacity will be taken up in existing (and any planned new) ICU capacity.
Hospitals do attempt to identify patients that are already suffering from AKI (“see and treat”), but this only creates marginal gains, and does not avoid blocking a bed that would otherwise be available to another patient. Prevention is critical.
Innovative, comprehensive solutions
Copeland Clinical AI (C2-Ai) has derived a simple to use App built around our unique, global referential dataset and derived from CRAB, the World’s most sophisticated patient safety system. The system is capable of identifying the 90 per cent of clinical variation/avoidable harm that a typical hospital’s own monitoring and reporting systems do not detect. The COMPASS Ai-backed tools support evidence-based, clinical decision making to assess and stratify patients by their individual risk of acquiring these conditions. It can provide results in 30 seconds on admission or change of conditions including recognised clinical pathway guidance on the steps to take to mitigate the risk and avoid the AKI/HAP.
The intuitive App allows selection of the setting – e.g. general medical, an orthopaedic unit or general surgical, and then with less than 10 tick-box clinical questions provides a specific risk of the condition occurring tailored to that patient.
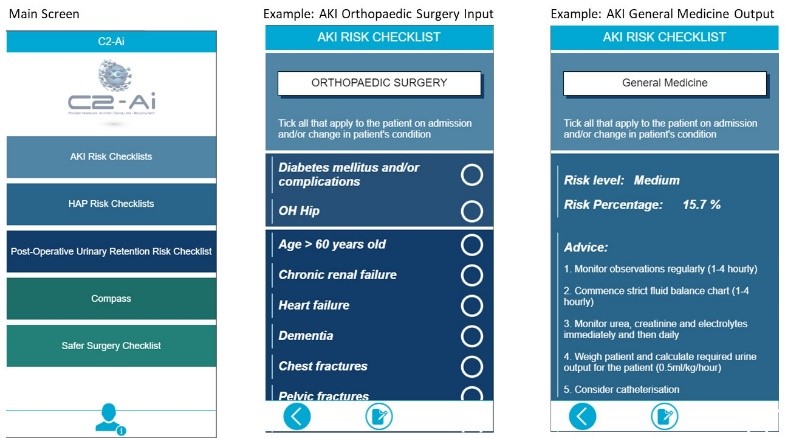
Clinicians choose from a simple list of key variables that they are all familiar with, eliminating the need for extensive form filling.
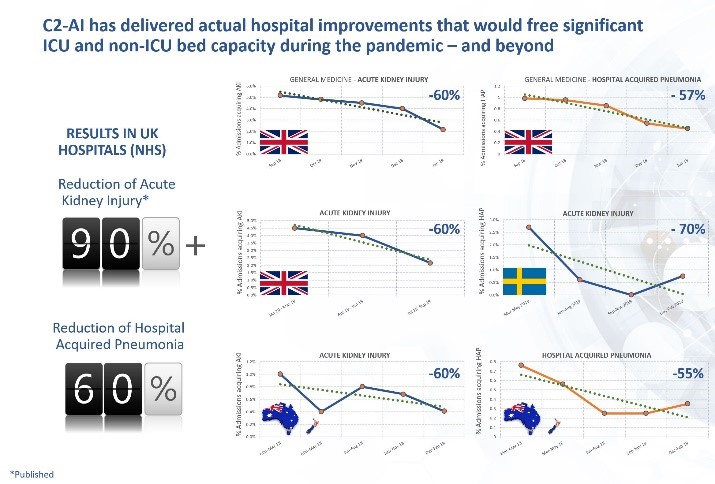
Application of C2-Ai’s most recent iteration of our approach in one site in England resulted in almost complete eradication of hospital acquired AKI within weeks. Another hospital using this approach reduced these conditions by 50 per cent in less than the first 2 months. In other case-studies, C2-Ai’s systems have consistently delivered hospital-wide, in-year reductions in AKI and HAP approaching 60 per cent and our approach has contributed to a Patient Safety Award.
These are secure mobile device applications that do not require any integration, patient IDs, complex training or an Internet connection and are available today.
An immediate deployment across NHS England with a 50 per cent reduction in these conditions would result in 90,000 ICU bed-days being freed in the following 3 months. That’s enough for an extra 11,250 Covid-19 patients, a further 300,000 inpatient bed-days saved and 18,000 lives saved just from the reduction of AKI/ HAP. Even in non-surge periods, those proven reductions would deliver £900 million of direct savings alone annually and save 75,000 lives relating to AKI and HAP.
For more information, visit c2-ai.com