
Restarting endoscopy: how can rising waiting lists be addressed?

What estate based solutions are there to address mounting backlogs across the NHS?
It is estimated that as many as 10 million people will be awaiting surgery by the end of 2020, but the suspension of services has also impacted on diagnostic test activity, leading to longer waiting times. What’s more, the low level of referrals in the last three months suggests there is a hidden backlog of patients that will add to diagnostic waiting lists in the coming months.
It is becoming clear that Covid-19 risk will be a feature in hospitals for the foreseeable future. As hospitals gradually reopen for planned procedures and tests, how can activity be upscaled while maintaining critical care capacity during a second wave or localised Covid-19 outbreaks? And how can we prevent waiting lists escalating beyond control?
Falling diagnostic activity
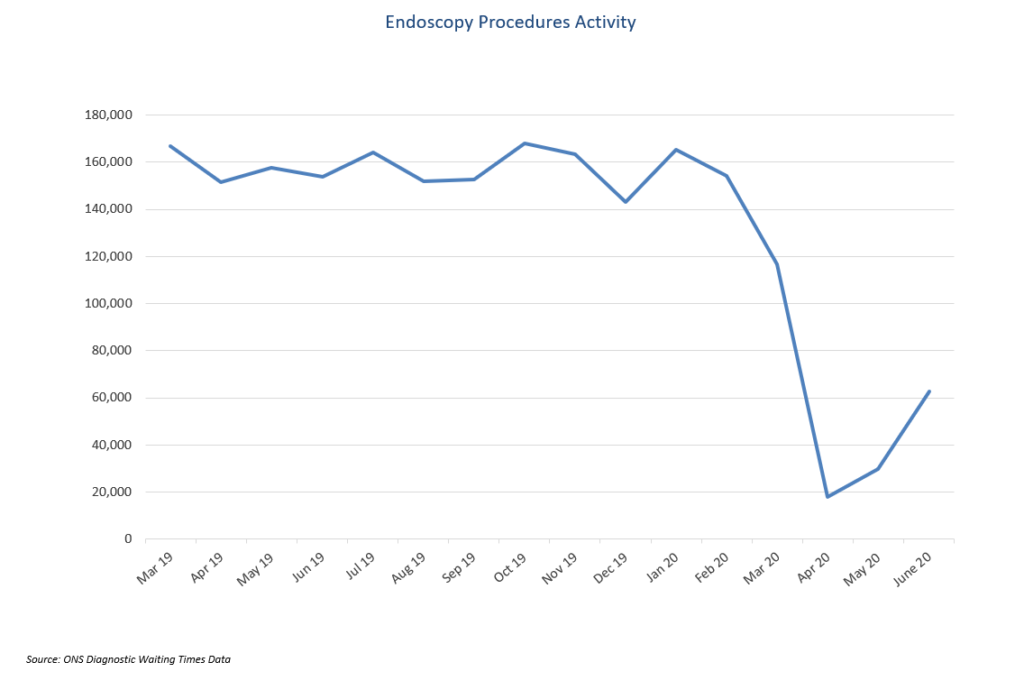
The pandemic’s impact on diagnostic testing activity was seen from February, when activity was slightly down, followed by a more significant fall in March, and an even steeper decline in April, as non-essential procedures were cancelled or postponed.
However, the total waiting list for diagnostic tests has not increased as expected – in fact, it declined from just over 1 million in February to around 750,000 in March, and remains below its pre-Covid level, as urgent tests have continued throughout lockdown. This emphasises the delayed referrals issue, which are expected to hit waiting lists in autumn.
In endoscopy, activity has fallen substantially. Official data shows that, although activity increased slightly in May 2020, of endoscopy numbers in the month fell substantially below normal and were over 80 per cent lower than in May 2019. While we are now seeing an increase in activity, endoscopy procedures are still way below pre-Covid levels.
The concern is that this fall will significantly impact gastrointestinal cancer diagnosis and treatment. Delays in cancer diagnoses can reduce treatment options and can be life-threatening, as late-stage diagnosis adversely affects mortality outcomes. This may also inflate the cost of cancer care given the additional treatments required for late-stage disease.
Endoscopy waiting lists are rising
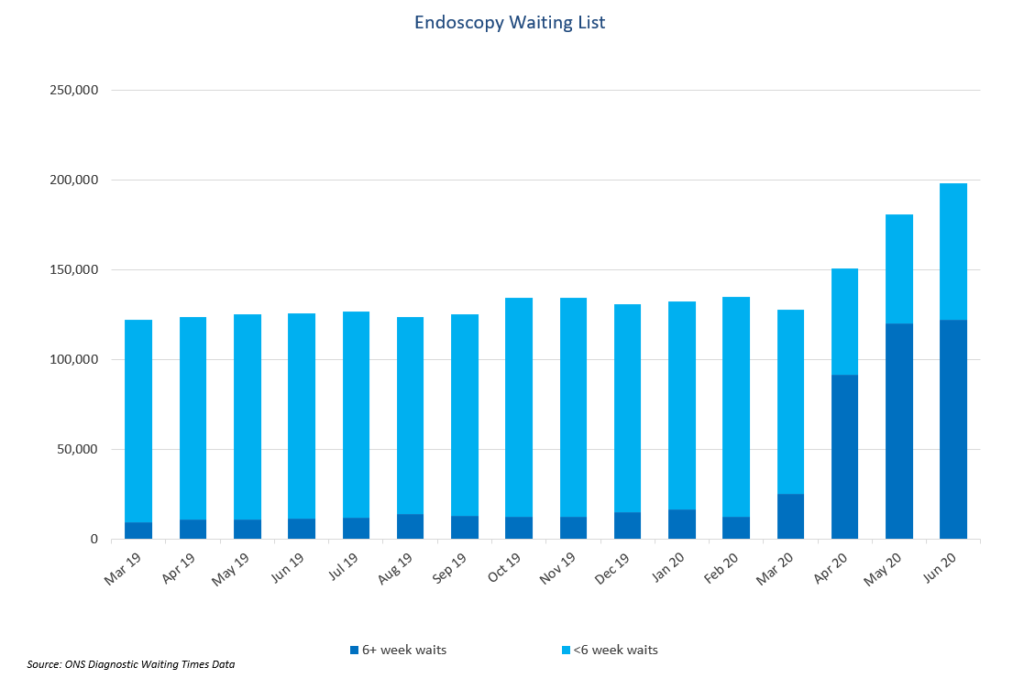
Most endoscopy procedures were suspended following the British Society of Gastroenterology (BSG) guidance at the end of March advising hospitals to suspend all non-emergency activity. Therefore, endoscopy waiting lists have increased throughout the pandemic, except for a slight dip in March.
In total, 180,000 patients were waiting for an endoscopy in England in May, and just under 200,000 in June, compared with the 120,000 to 130,000 baseline over the past year. Whilst we have yet to see the full impact on the numbers waiting for a procedure, the impact on waiting times has been immediate.
Around 66 per cent of those on the waiting list, approximately 120,000 patients, had been waiting more than six weeks for an endoscopy in May 2020 – against a target of 1 per cent, and 9 per cent in May 2019. And this ignores delayed referrals.
The speed of restarting procedures can have a huge impact, since new patients join the waiting list each week, and the wait for those already on it is increased. NHS trusts face major practical challenges in restarting endoscopy and, so far, the restart has been slow.
Restarting endoscopy
Public Health England has mandated at least three air changes between patient procedures within endoscopy procedure rooms, and this, plus additional cleaning, extra time changing in and out of enhanced PPE and social distancing has affected the number of patients able to be treated. It is widely estimated that productivity is reduced by up to 50 per cent.
Both NHS England (NHSE) and the BSG have advocated separating Covid-19 and non-Covid patients, to minimise risk and reintroduce elective procedures safely. Trusts have been urged to establish ‘cold’ or ‘Covid-minimised’ sites, ideally as a stand-alone facility with separate patient and staff access to the rest of the hospital. By providing planned services from a ‘cold’ site, infection risk can be mitigated and capacity protected from the risk of last-minute postponement or cancellation.
In a ‘Covid-minimised’ environment, strict patient flows separate potentially Covid-19 positive patients from others. BSG guidance suggests the facility should have linear patient flows with separate entrances and exits, and that staff rotation between ‘hot’ and ‘Covid-minimised’ areas should be avoided.
Establishing a ‘cold’ site
One of the best ways to achieve this separation is to use an external building as a ‘cold site’. This approach also reassures patients who may be concerned about attending a hospital with Covid-19 patients, that attending an endoscopy appointment does not increase their Covid risk.
Creating a ‘Covid-minimised’ environment presents a significant challenge for many trusts; some do not have buildings or other sites they can use. Trusts with fewer sites and those with high-rise or older buildings face a particular challenge.
The underused Nightingale hospitals have been suggested as ‘cold’ sites to boost capacity for elective procedures, but this would depend on suitability, and could mean long journeys for patients, who might be shielding or have other health conditions. Additional, temporary staff might also be needed.
A more practical way to safely restart procedures is flexible healthcare solutions. Mobile endoscopy suites, for example, have separate entrances and exits, built-in recovery-ward space and decontamination facilities, and can be configured with a separate reception, staff rest areas and changing rooms.
Mobile or modular endoscopy suites can rapidly be set up to provide a complete, self-contained, separate ‘cold’ site. These can be situated on the main hospital site, eliminating patient transfer, minimising Covid-19 risk and reassuring patients that it’s safe to attend.
Temporary units can also be supplied with experienced, adequately trained clinical staff.
Improvements to efficiency will be extremely difficult while productivity is much lower than normal, but throughput could be increased by scheduling changes to maximise the use of existing procedure rooms. Although the current restrictions lengthen downtime between cases, earlier starts, later finishes, weekend or even 24-hour operation could be considered. Insourcing staff could make this viable.

Endoscopy cold sites
In Scotland, where around 19,000 people are waiting for an endoscopy, the Government is restarting services with mobile endoscopy units. Flexible healthcare solutions are also used as ‘cold’ sites at across England.
At one Midlands hospital, a mobile endoscopy unit supplied by Vanguard Healthcare Solutions was already operating, and proved ideal for the safe resumption of two-week wait endoscopy procedures.
Although the unit needed minimal modification, working practices needed adaptation. No known Covid-19 patients are booked in, and all patients are screened prior to attending with a physical temperature check on arrival.
The Trust has found that patients feel more comfortable attending for procedures as the mobile unit is away from the main building, and it has its own staff, who are not circulating throughout the hospital, which helps ensure the unit remains a ‘cold’ site. This facility has been instrumental in resuming endoscopy procedures,and more than 200 patients have since been seen.
Elsewhere, the Medway NHS Foundation Trust found internal capacity limited due to new medical rotas and staff self-isolating. Endoscopy services demand was already high before Covid-19, and during the outbreak the Trust’s waiting list was growing by more than 60 patients a week.
The Trust has a single site with no spare space for. At the onset of the Covid-19 crisis, the Trust was already working with 18 Week Support and the Will Adams Treatment Centre (Care UK), to manage endoscopy referrals in a separate location, and this site was adapted to provide a ‘Covid-minimised’ facility for endoscopy, with 18 Week Support providing clinical staff and advising on a safe patient pathway.
Paula Tinniswood, Director of Improvement at Medway NHS Foundation Trust, said: “With the abrupt cessation of all but very urgent endoscopic diagnostics across the NHS, Medway’s leadership team decided to continue the existing partnership arrangement to support patient care as a ‘cold’ site.
“All stakeholders were asked to sign and authorise the pathway, which included Covid-swabbing, PPE usage and triage against criteria. This approach ensured that patients on two-week wait cancer pathways continued to be seen in a safe manner.”
An urgent need to boost capacity
It is likely that the need to care for Covid-19 patients or maintain a level of preparedness will remain for some time, possibly into next year. Given that productivity will be reduced during this time, significantly impacting on capacity and the expected influx of new referrals, endoscopy waiting lists are likely to increase for the foreseeable future.
Using the 2019 figures, the estimated backlog in referrals during March to May could be around 270,000, with June referrals also set to remain low. This will have a substantial impact on waiting lists in the coming months, as primary care resumes and referral levels start to increase towards normal.
Dr Matthew Banks, 18 Week Support Clinical Lead for Gastroenterology, said: “The sooner elective care can be restarted, the less severe the future impact will be. The urgent need is to find ways to increase diagnostic activity as quickly, and safely, as possible. A surge in gastrointestinal cancer referrals is expected over the next few months, and the impact on patients could be severe.”
‘Cold’ sites are likely to be essential for managing waiting lists until the pandemic is over. But even post Covid-19, waiting times will be substantial and more capacity will be needed. Flexible infrastructure and staffing solutions, such as those from Vanguard and 18 Week Support, can be set up quickly to provide hospitals with additional capacity and support, in any location.
A paper on restarting endoscopy can be downloaded from www.vanguardhealthcare.co.uk or 18weeksupport.com.